From breakthrough science to operational reality
Advanced Therapy Medicinal Products (ATMPs), including cell and gene therapies, are transforming personalized medicine. Once patient-specific therapies are developed and approved, their medical potential depends on a demanding operational condition: they must reach the patient on time, clearly assigned, regulatorily compliant, and executed under control.
In a 2023 survey of more than 500 manufacturers, 83% reported having ATMPs in their pipeline. At the same time, commercialization is still early in “pharma scale” terms: global spending on cell and gene therapies reached $5.9B in 2023 but remains only a small fraction of global medicine spending (~1%). However, Public FDA/EMA lists show a market that is expanding but still concentrated: ~45 distinct approved products across ~40 companies worldwide. This combination (rapid innovation and early-stage commercialization) is exactly where operational execution becomes a differentiator.

Why Vein to Vein process & Batch size “one” is critical?
Many pharma companies are advancing ATMPs, but manufacturing and supply chain are still shaped by manual process components, limited scalability, consistency risks, and narrow time windows.
The fact that about 20 percent of patients die while waiting for CAR-T cell therapy cannot be attributed solely to digital process weaknesses. The figures show why improvements in process quality, data management, coordination, and release time are directly relevant.
ATMP processes follow a strict make-to-order logic: one patient request, one batch, one therapeutic time window.
There are no safety stock and no later interchangeability. Even minor disruptions can cascade into missed manufacturing slots, delayed infusion appointments, or in the worst case, loss of a time‑critical therapy opportunity.
This logic increases the requirements for control and traceability.
Two control concepts sit at the center of the vein-to-vein process:
- Chain of Identity (COI): COI (Chain of Identity): Ensures the therapy is uniquely matched to the correct patient from collection through manufacturing to reinfusion (patient ↔ starting material ↔ final product).
- Chain of Custody (COC): the record of who was responsible when across every handover (clinic, logistics providers, CDMO/manufacturer, QA/QP release, and back to the clinic).
In practice, this means ATMP success depends on end-to-end orchestration across multiple independent organizations and systems.
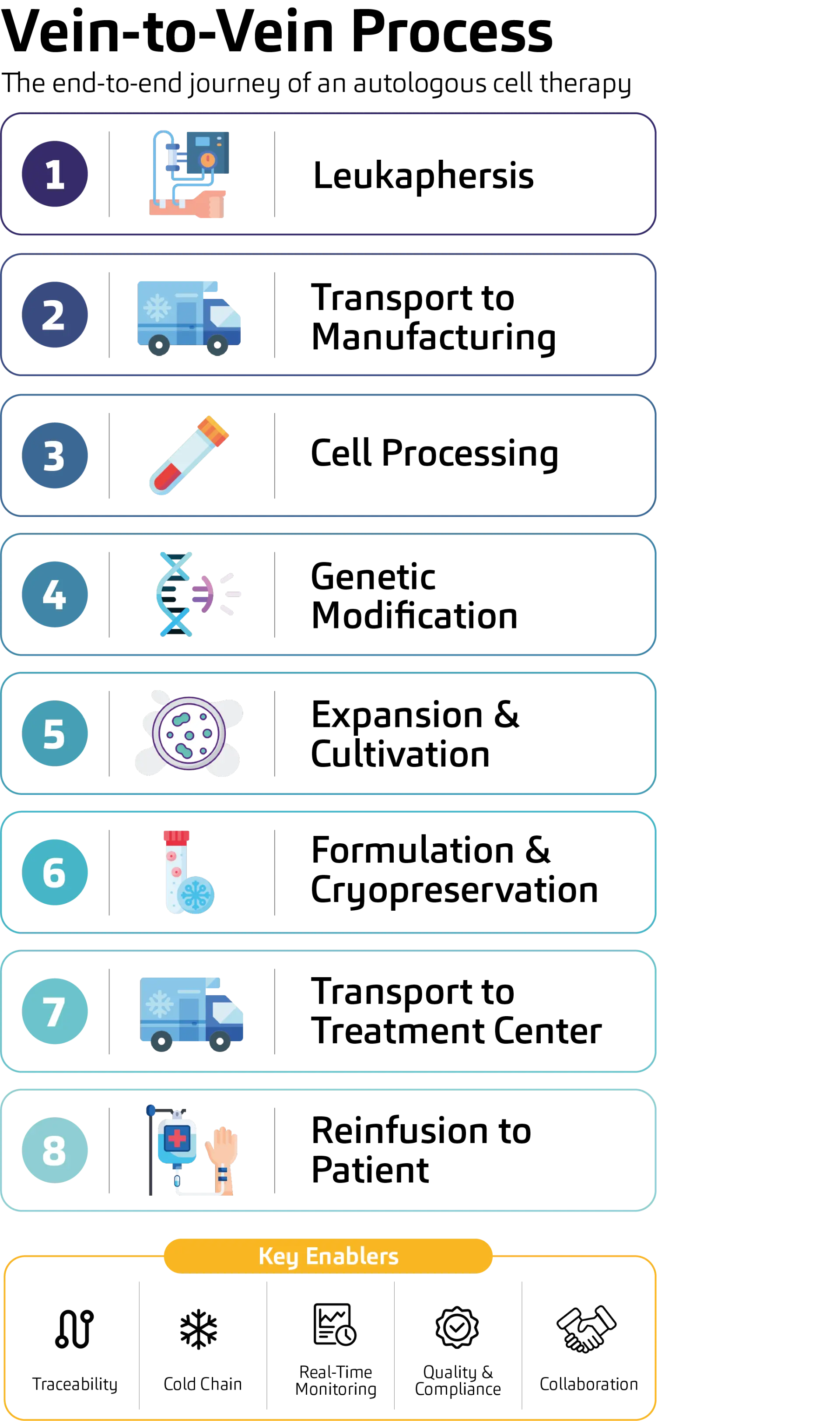
From collection to infusion: the key steps in the cell and gene therapy pathway.
From manual coordination to controlled data orchestration
Because the vein‑to‑vein process is inherently multi‑partner, the most effective lever is not “one more tool,” but data continuity, clear data ownership, and governance across organizational boundaries. In practice, many delays and risks are created when critical information is split across core IT systems (ERP, MES, LIMS, QMS), logistics platforms, and clinic systems, without consistent identifiers, rules, and responsibilities.
A proven pattern is an event-based “patient-batch record”: a governed data object that connects clinical milestones, logistics events, manufacturing execution, quality results, and release status into one coherent timeline. In this context, event-based control means it is not enough to know that a step happened. You need to know what happened, when it happened, under which conditions, who owned each handover, which patient identity it belongs to (COI/COC), and whether the evidence required for QA/QP release is complete, consistent, and audit ready.
Compliance as a property of the entire network
ATMP digitalization touches classic GxP requirements (e.g., EU GMP Annex 11, 21 CFR Part 11, ALCOA+ data integrity), but it also expands into third‑party platforms, cloud components, cross‑company interfaces, NIS2/KRITIS, and GDPR. As integrations increase, validation scope and audit trail reconstruction complexity grows. This is why a risk‑based validation strategy is essential: it focuses effort where it matters most, on the data objects, interfaces, and controls that influence patient safety, product quality, and release decisions.
Resilience needs a similar shift. In a vein‑to‑vein environment, cyber incidents and outages are not only IT topics, they can disrupt a time‑critical clinical pathway. Traditional Business Continuity / Disaster Recovery (BC/DR) often focuses on restoring systems; ATMPs require continuity planning designed around the patient‑critical path and partner dependencies.
From process to availability
ATMPs show that medical progress creates new requirements for industrial processes. Personalized medicine will become operationally manageable only if its process and data infrastructure keeps pace with medical innovation, so speed, safety, compliance, and availability work together.
The pragmatic way forward is to combine a targeted process/data assessment with a set of execution steps:
- Map the vein‑to‑vein process as a critical path (not as separate departmental workflows).
- Define the patient‑batch data model and assign system‑of‑record ownership for IDs and states (patient, collection, batch, shipment, release).
- Create an event catalogue + exception taxonomy (what can go wrong, how detected, who acts, what evidence is required).
- Establish integration governance (API strategy, interface ownership, audit trail approach across partners).
- Embed compliance‑by‑design with a risk‑based validation approach from day one (focus on evidence and integrity, not documentation volume).
- Design ecosystem resilience around the patient path (partner dependencies, continuity for critical events, escalation playbooks).
Authors
Would you like to learn more about this topic or discuss individual challenges?
Our contacta are available for a personal consultation.